CONGRATS! YOU EARNED FREE SHIPPING.

Product Title
1
$0
$0
Subscription Title

Looking kind of empty in here.
We recommend:

Get advanced insights into symptoms, fertility, and other health outcomes. Prelim results in 1-3 days.

Progesterone in perimenopause: learn when to use it, how much to take, and what to expect for sleep, hot flashes, bleeding, and hormone balance.
Words by Olivia Cassano
Scientifically edited by Dr. Krystal Thomas-White, PhD
Medically reviewed by Dr. Kate McLean MD, MPH, FACOG
Key takeaways:
Perimenopause can feel like a rollercoaster: one month, your period might arrive early and be heavy; the next month, you might struggle to sleep; and suddenly, you find yourself sweating through your pajamas in the middle of winter. Many of these changes occur because your body produces less progesterone as ovulation becomes less regular.
Because of this, hormone therapy containing progesterone can be a helpful option for many women navigating perimenopause. It’s not just for women on estrogen; progesterone on its own can support sleep, calm nighttime anxiety, steady bleeding patterns, and even reduce hot flashes and night sweats. Keep reading to learn more about what progesterone does, who benefits most, and when to take progesterone for perimenopause.
During your reproductive years, progesterone rises only if you ovulate. Ovulation triggers the formation of the corpus luteum, which releases progesterone during the luteal phase (the second half of your cycle). In perimenopause, ovulation becomes erratic. Some cycles you ovulate early, some late, and some not at all. When ovulation doesn’t happen, your body simply doesn’t produce much progesterone.
Low or inconsistent progesterone means estrogen often has the upper hand. Even if estrogen levels are also changing, they can remain relatively higher compared with progesterone, creating what many describe as estrogen dominance. It’s not that there’s too much estrogen; it’s more about having not enough progesterone to keep things balanced.
You may notice low progesterone symptoms like heavy or prolonged periods, breast tenderness, irritability, spotting between periods, and sleep disturbances. Progesterone typically has a calming effect on the brain, so when levels drop, many women feel more anxious, restless, or sensitive to stress, especially at night.
Progesterone therapy aims to replace or supplement what your body isn’t reliably making. By adding back some of that steadying influence, many women experience smoother cycles, better sleep, and fewer disruptive perimenopause symptoms.

Recurrent symptoms? Get Evvy's at-home vaginal microbiome test, designed by leading OB-GYNs.
Progesterone isn’t only for women using estrogen, although it is essential for endometrial protection if you take systemic estrogen and still have a uterus. Many women use progesterone alone during perimenopause because it targets some of the most bothersome perimenopause symptoms.
People who may benefit include:
This is the most common and best-studied form of progesterone for perimenopause. It’s taken as a capsule (usually 100–300 mg at bedtime) and has been shown in randomized trials to improve sleep, reduce night sweats and hot flashes, and support mood. Another benefit is that progesterone protects the endometrium when used alongside estrogen. Because it can be calming and mildly sedating, bedtime dosing is ideal. Many women find it both effective and gentle, with fewer metabolic or cardiovascular side effects than synthetic progestins.
Used more often in fertility care, vaginal progesterone can still play a role in perimenopause when targeted endometrial support is needed or if someone doesn’t absorb oral forms of progesterone well. It delivers the hormone directly to the endometrium, which can be useful for bleeding issues. However, it isn’t well-studied for improving sleep or managing vasomotor symptoms, and some women find the application messy or inconvenient.
While technically a synthetic progestin rather than natural progesterone, a hormonal IUD is commonly used in perimenopause for endometrial protection and to control heavy or irregular bleeding. It releases a very small amount of hormone locally, making it highly effective with minimal systemic side effects. Many women appreciate the “set it and forget it” convenience. However, it doesn’t offer benefits for sleep, anxiety, or hot flashes.
Despite their appeal, OTC creams typically deliver very low and unreliable progesterone levels. They may moisturize the skin, but don't ease perimenopause symptoms, nor do they protect the endometrium if you’re on estrogen therapy. For medical use, clinicians rarely recommend them because absorption varies too widely to be dependable.
When it comes to progesterone in perimenopause, providers almost always start with bedtime dosing and adjust based on sleep, bleeding patterns, and symptom relief.
Most regimens use oral progesterone (generally 100–300 mg) because it has the strongest evidence for improving sleep and reducing hot flashes and night sweats while maintaining an excellent safety profile. The “right” regimen depends on whether you want steady symptom control, predictable withdrawal bleeding, or are combining progesterone with estrogen therapy.
Higher doses, like 300 mg nightly, are sometimes recommended when sleep disruption or hot flashes are more severe. Your clinician may fine-tune your dose after a few cycles to balance the benefits with any side effects, such as grogginess or spotting.
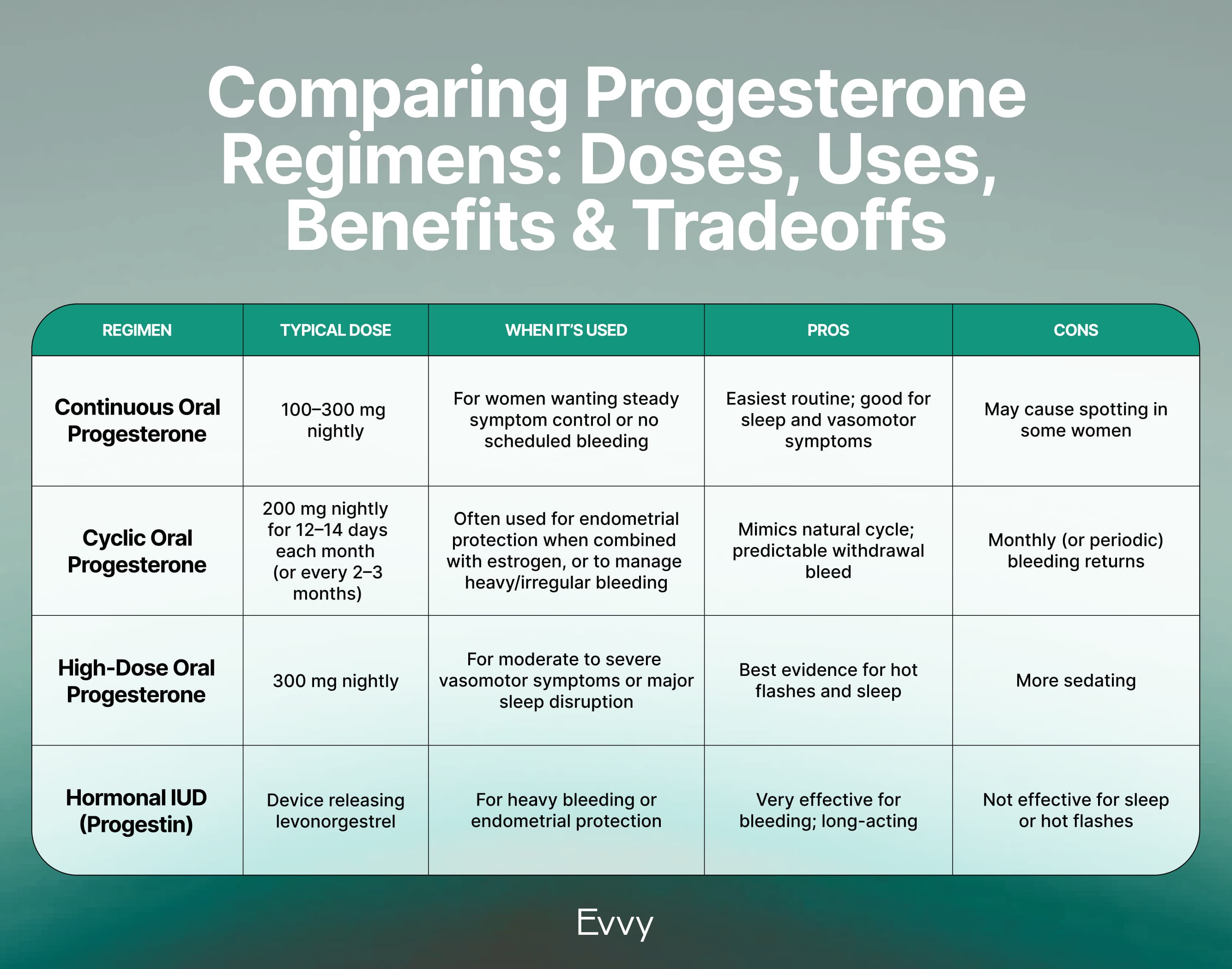
A few important points to keep in mind: progesterone is usually taken at bedtime because it can cause drowsiness, which actually helps support sleep. While some women do well on lower doses, most of the research showing clear benefits uses doses between 200 and 300 mg. Your clinician may adjust your dose over time based on how your bleeding patterns, sleep quality, or mood respond to treatment.
Choosing between continuous and cyclic dosing depends on your symptoms, your cycle patterns, and your personal preferences.
If your periods are very irregular, continuous dosing can feel simpler. But if you’re specifically targeting bleeding or using estrogen therapy, a cyclic schedule might be preferable.
In practice, both approaches can work well. Your healthcare provider will help you decide based on what’s most important to you: steady symptom relief, predictable bleeding, or syncing with estrogen therapy.
Yes, you can use progesterone on its own during perimenopause. Many healthcare providers start with progesterone when estrogen isn’t desired or isn’t well-tolerated. Progesterone monotherapy can improve sleep, reduce nighttime anxiety, and even decrease hot flashes and night sweats. It can also help regulate bleeding and ease luteal-phase symptoms.
That said, progesterone alone doesn’t replace the benefits of estrogen for things like bone density, vaginal dryness, or the more intense vasomotor symptoms some women experience. So while it may help a lot, it won’t solve everything.
Monitoring also matters. Because progesterone affects the endometrium and the menstrual cycle, clinicians closely monitor how your bleeding patterns change. Unexpected spotting, heavier periods, or new symptoms may signal the need for adjustments — either in dose, timing, or adding estrogen later on.
For the right person, though, progesterone alone can be a meaningful and effective bridge through the roller-coaster years of perimenopause.
Progesterone is generally well-tolerated, especially oral micronized progesterone, which has a favorable safety profile compared with synthetic progestins. It’s less likely to cause metabolic or cardiovascular side effects, and studies show minimal risk of depression or serious adverse events.
Common side effects include:
Progesterone therapy isn’t suitable for everyone. Women with a history of progesterone-sensitive breast cancer or endometrial cancer should speak carefully with their oncologist. Those with severe liver disease or certain clotting disorders may also need alternative options. And women without a uterus may not need progesterone unless there’s another medical reason, such as managing endometriosis.
As with any hormone therapy, the key is individualization. Finding the lowest effective dose, used for the shortest duration necessary, with regular check-ins to be sure it’s still the right fit.
When you start progesterone, it’s helpful to track your sleep, mood, hot flashes, and bleeding for the first few months. Many women notice improvements in sleep within the first week or two, while changes in bleeding patterns may take a cycle or two to settle.
Doctors often adjust the dose if sleep is still unsettled or if you feel too groggy the next morning. If heavy bleeding continues, a shift to a cyclic regimen or adding an IUD may help.
Monitoring bleeding is especially important. Irregular spotting can be normal at the beginning, but heavy or persistent bleeding needs follow-up. This isn't usually a sign of something serious, but it can point toward the need for a different regimen.
As helpful as it is, progesterone isn’t a “set it and forget it” therapy, so regular conversations with your doctor help make sure you're getting the best possible benefit with the fewest downsides.
There’s no single age or deadline for stopping progesterone. The decision depends on your symptoms, whether you’re still menstruating, whether you're using estrogen, and how you feel overall.
Many women stop cyclic progesterone once they go a full year without a period, one marker that menopause has arrived. But if you’re taking progesterone for sleep, hot flashes, or anxiety, you may want to continue beyond that point. If you’re using systemic estrogen and still have a uterus, you’ll need to continue some form of progesterone for as long as you use estrogen.
It’s also fine to try tapering off after your symptoms settle and see how you feel without it (just be sure to consult your provider before doing so). Some women discover they no longer need progesterone; others choose to continue because the benefits (especially for sleep) remain meaningful.
The guiding principle for hormone therapy is simple: reevaluate periodically with your clinician. Your needs at 45 may look totally different at 52, and that’s normal.
Yes. Progesterone is usually the first hormone to shift during perimenopause because it depends on consistent ovulation, and ovulation becomes more unpredictable in the late 30s and 40s. Some cycles produce a normal amount, others produce too little, and some don’t produce any at all. This inconsistency can show up as sleep issues, mood swings, spotting, or heavier bleeding. These fluctuations often start years before estrogen levels begin their more dramatic rise and fall, which is why many women feel “off” well before menopause officially arrives.
Low or fluctuating progesterone levels can create a mix of physical and emotional symptoms. Many women notice sleep disturbances, particularly waking up in the middle of the night with a sense of restlessness or anxiety. Others experience breast tenderness, headaches, mood swings, heavier or more prolonged periods, or spotting between cycles. These symptoms often come and go because your progesterone levels change from month to month. While they can feel unsettling, they’re extremely common during the menopause transition.
For many women, yes. Progesterone therapy can be especially helpful for improving sleep, calming nighttime anxiety, regulating bleeding, reducing hot flashes and night sweats, and easing luteal-phase mood symptoms. Studies show that 300 mg of oral progesterone can reduce moderate to severe vasomotor symptoms with a strong safety profile. It’s also essential for women with a uterus who take estrogen, since it protects the endometrium. However, progesterone isn’t a universal solution, and therapy should be individualized based on menopause symptoms and health history.
Progesterone itself doesn’t cause weight loss, and it isn’t recommended for that purpose. However, some women find that better sleep and calmer moods help them make healthier choices, manage their appetite more easily, or reduce stress-related eating. Others may feel less bloated when their cycles become more regulated. Still, these changes are indirect effects and not guaranteed. Weight gain in perimenopause is influenced by many factors — hormone levels, sleep, stress, muscle mass, and metabolism — so progesterone is only one small piece of the larger picture.
Yes, and many women do. Continuous nightly dosing is simple and can provide steady benefits for sleep and vasomotor symptoms. It also avoids the scheduled monthly withdrawal bleed that comes with cyclic regimens. Some women may still experience spotting at first, but this often improves over time. Continuous dosing is especially useful for women whose cycles are unpredictable or mostly anovulatory. As always, your provider may adjust your dose or schedule depending on how your symptoms and bleeding patterns respond.
The most commonly used doses are 100–300 mg of oral micronized progesterone at bedtime. Research supporting improvements in hot flashes and sleep quality typically uses 300 mg, but many women do well on 100-200 mg. The right dose depends on your symptoms, bleeding patterns, and how sensitive you are to drowsiness. Clinicians generally aim for the lowest effective dose and reassess periodically to see whether adjustments (or stopping altogether) are appropriate. It’s normal for needs to change as you move further into the menopause transition.








.avif)